new web: http://bdml.stanford.edu/pmwiki
TWiki > Haptics Web>StanfordHaptics>HapticsForGaitRetraining (07 Jun 2011, MarkCutkosky)
Haptics Web>StanfordHaptics>HapticsForGaitRetraining (07 Jun 2011, MarkCutkosky)
Overview
Haptics for Gait Retraining grows out of the MotionDisplayKAUST project, and focuses on a motion training application of particular clinical importance. This project is aimed to explore the potential of gait retraining as a knee osteoarthritis treatment. We use haptic feedback, through vibration and skin stretch, along with visual and auditory feedback, to assist in training new walking strategies. The project is currently supported by the National Science Foundation under grant 1017826. Additional work is summarized in the page by P. Shull on Data Driven Movement RetrainingBackground
Knee Joint Loading and the Knee Adduction Moment
 Osteoarthritis is a widespread disease that commonly affects the medial compartment (inside) of the knee joint. It has been shown that shifting the loading from the medial compartment to the lateral compartment (outside) of the knee joint is effective for preventing and treating knee osteoarthritis.
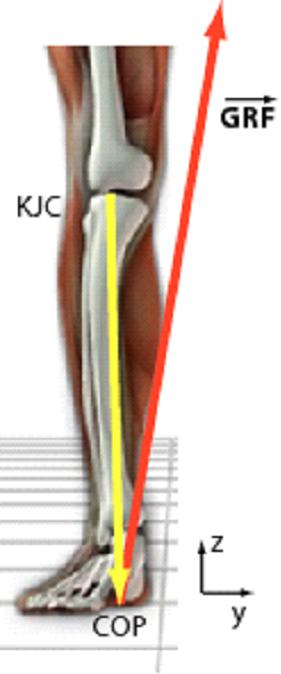
The common way of measuring knee loading is the knee adduction moment. This value is calculated by taking the cross product of the ground reaction force (GRF) and the position vector from the knee joint center (KJC) to the foot's center of pressure (COP) and keeping the component of the computed moment in the direction pointing directly away from the surface of the patella (kneecap).
We use multiple haptic devices to retrain patients and healthy subjects to walk with a reduced knee adduction moment gait to explore its value for knee osteoarthritis treatment.
Additional background information can be found here.
Osteoarthritis is a widespread disease that commonly affects the medial compartment (inside) of the knee joint. It has been shown that shifting the loading from the medial compartment to the lateral compartment (outside) of the knee joint is effective for preventing and treating knee osteoarthritis.
The common way of measuring knee loading is the knee adduction moment. This value is calculated by taking the cross product of the ground reaction force (GRF) and the position vector from the knee joint center (KJC) to the foot's center of pressure (COP) and keeping the component of the computed moment in the direction pointing directly away from the surface of the patella (kneecap).
We use multiple haptic devices to retrain patients and healthy subjects to walk with a reduced knee adduction moment gait to explore its value for knee osteoarthritis treatment.
Additional background information can be found here.
System
Gait Retraining
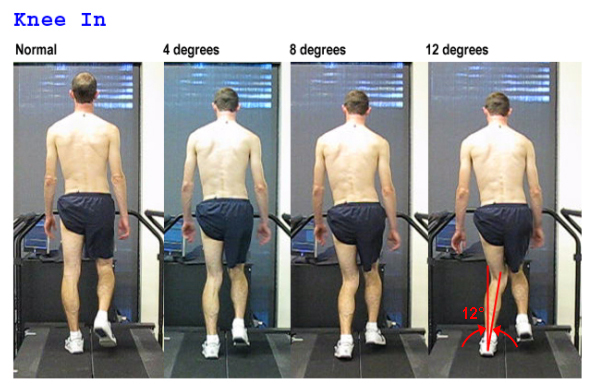
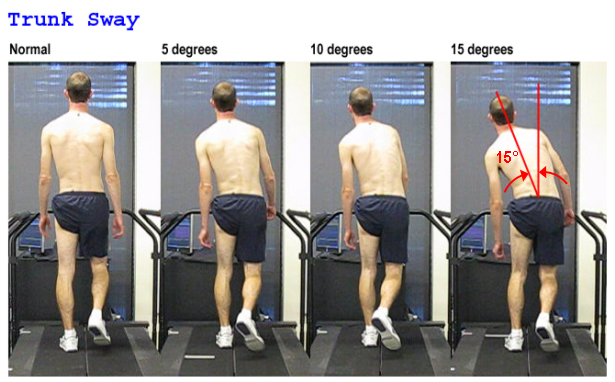
Subjects are taught to modify three different gait parameters, which have previously been shown to reduce knee adduction moment. These parameters include foot progression angle (toe in or out), tibia angle (knee in), and trunk sway angle. Gait retraining can either be explicit or implicit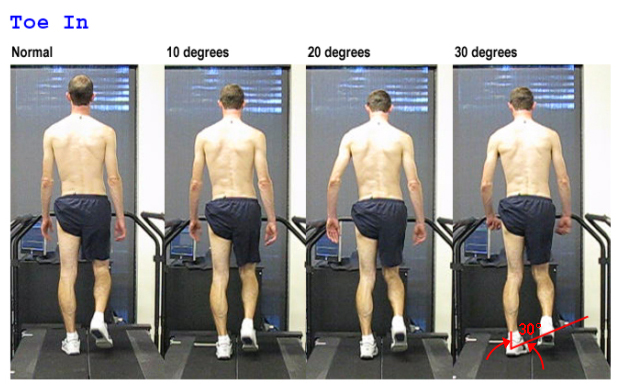

Haptic Feedback
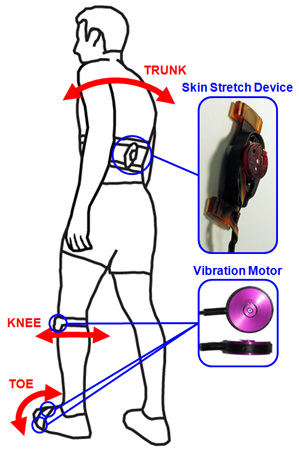 We use vibration and skin stretch haptic feedback to inform the gait parameters. Although we are still exploring optimal ways to provide haptic feedback, one approach is described that has been adequate for some of our past experiments.
The desired foot progression angle is indicated with two vibration motors - one on the medial side (inside) of the foot and one on the lateral (outside) of the foot. If the foot progression angle is too large the lateral vibrotactor is activated and if the foot progression angle is too small the medial vibrotactor is activated.
The desired tibia bone angle, measured from a vertical line, is indicated by one vibration motor placed on the lateral side of the knee. If tibia angle is too small the motor is given a constant vibration and if the angle is too large the motor is given three short vibration pulses.
The desired backbone angle is indicated by either a skin stretch device placed on the lower back or two vibration motors place on either side above the hips.
We use vibration and skin stretch haptic feedback to inform the gait parameters. Although we are still exploring optimal ways to provide haptic feedback, one approach is described that has been adequate for some of our past experiments.
The desired foot progression angle is indicated with two vibration motors - one on the medial side (inside) of the foot and one on the lateral (outside) of the foot. If the foot progression angle is too large the lateral vibrotactor is activated and if the foot progression angle is too small the medial vibrotactor is activated.
The desired tibia bone angle, measured from a vertical line, is indicated by one vibration motor placed on the lateral side of the knee. If tibia angle is too small the motor is given a constant vibration and if the angle is too large the motor is given three short vibration pulses.
The desired backbone angle is indicated by either a skin stretch device placed on the lower back or two vibration motors place on either side above the hips.
Human Performance Laboratory Setup
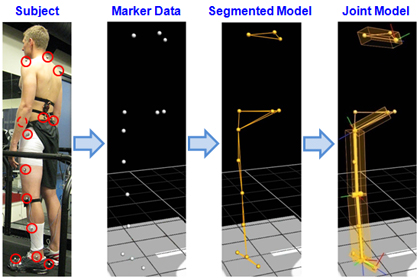 A motion capture system and treadmill instrumented with force plates are used to calculate knee adduction moment and track movement.
A motion capture system and treadmill instrumented with force plates are used to calculate knee adduction moment and track movement.
Additional details about system implementation can be found here.
Experiments and Results
Experiments and results from a few of our major efforts are summarized on the following pages: Haptics Symposium 2010 Journal of Biomechanics Paper Preparation HCI Course ProjectAdditional Info
Portable System Human Tracking Frequencies Haptic Feedback Design Virtual PebbleIdeas, requests, problems regarding TWiki? Send feedback